In this COPD case study, we outline how to use the GOLD guidelines to guide medication therapy. Here’s the case!
KE is a 71-year-old male who has a history of cigarette smoking for 50+ years, COPD, cardiovascular disease, hypertension, peripheral arterial disease, GERD, and osteoarthritis. His primary concern is his breathing and COPD. He presents to the primary care clinic reporting that he is using his albuterol inhaler a bit more than he used to. Upon review of dispensing records, you note that this is accurate as he has increased the frequency of albuterol refills. While he notes a worsening of symptoms, he has not been hospitalized recently for COPD.
Upon assessment of his symptoms, a COPD assessment test (CAT) and Modified Medical Research Council dyspnea scare (mMRC) are performed. His CAT score was 14 and the mMRC was 3. Using our free COPD Cheat Sheet of the GOLD guidelines from pyrls.com (sign up for a free account and you can get the full COPD PDF cheat sheet along with many others), you can see that this patient would fall into category B when it comes to initiation of pharmacotherapy.
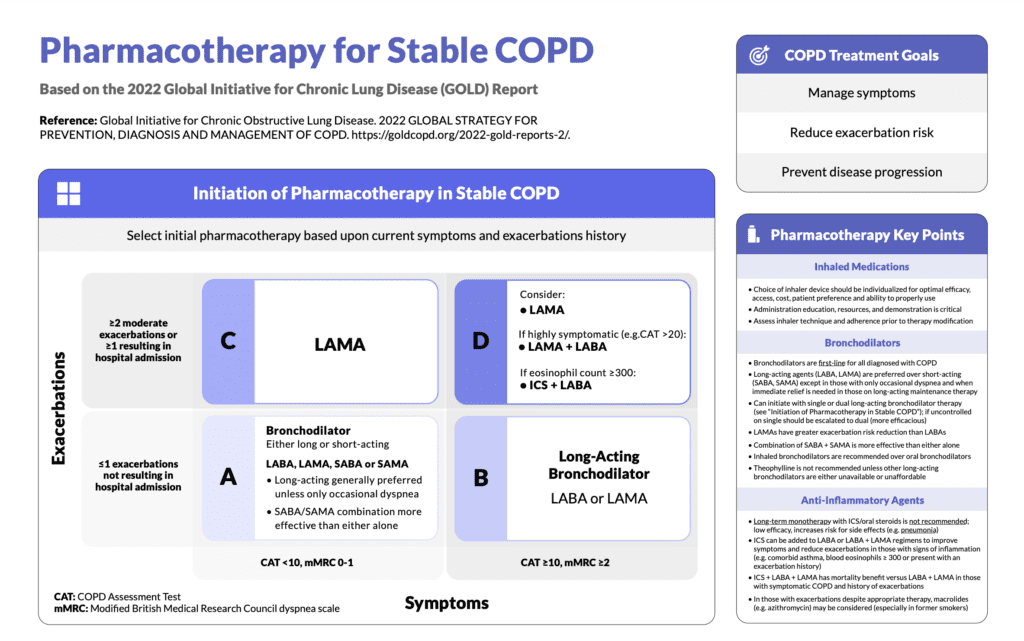
If a patient falls into category B, what medication would I choose? We have two options per the guidelines in that we can choose a long-acting beta-agonist or a long-acting anticholinergic (or antimuscarinic). While patient preference should be considered, my sense in COPD is to go with LAMA if all other things are being equal. This is what I have most frequently seen in practice as well. LAMA therapy has shown slightly better exacerbation risk reduction than LABAs as a whole.
We have a significant number of LAMAs now on the market whereas several years ago, we really only had one in tiotropium. Here’s the list of those agents.
- Aclidinium (Tudorza Pressair)
- Glycopyrronium (Seebri Neohaler)
- Tiotropium (Spiriva)
- Umeclidinium (Incruse Ellipta)
- Revefenacin (Yupelri) – nebulized formulation
If time was not an issue in educating this patient, it would be ideal to take the time to go through these devices and see which one the patient is more comfortable with so we don’t end up with situations like these. This could help guide selection and improve adherence. In reality, the LAMA of choice is often dictated by the insurance coverage that the patient has. In my practice and in my region of the country, I see tiotropium and umeclidinium as the most frequently used LAMAs. You wouldn’t likely use the nebulized formulation (revefenacin) unless there were concerns with the patient’s ability to deliver the dose via one of the other devices.
The last point I’d like to make in this COPD case study is to at least address smoking cessation. The patient may not be ready to quit as he has an extremely long history of use, but it at least should be mentioned.






